
Migraines and Headaches: A whole body approach
Migraines and headaches are among the most common neuro-vascular disorders, affecting millions worldwide (6). It is commonly treated with a tablet of paracetamol, as if it were nothing. But when this becomes so regular, weekly or even daily for some, is the paracetamol tablet the best long-term solution? Although paracetamol is considered safe, it is not completely harmless. It is increasingly recognised as an additional burden on the liver and on brain health. Most importantly, it does not fix the cause. As a naturopath and former chronic headache sufferer, I see how headaches are closely linked to lifestyle factors such as sleep, stress, and dehydration, as well as deeper physiological imbalances in the liver or the gut. This post explores definitions, physiology, and holistic management strategies for getting rid of these chronic headaches.
Migraine and Headaches: A neurovascular disorder
Headaches can be classified as tension headaches, migraines or also cluster headaches, the latter being less prevalent but intense episodes of debilitating pain nevertheless. Previously thought to be purely vascular, headaches are now understood as neurovascular disorders, meaning they involve a complex interplay between nervous and vascular systems. The neurological processes may even be the primary drivers, with vascular changes being a secondary response or a part of the overall neurovascular event.
Here's a bit more about the processes that make us feel so much pain and make the scientific community think both neurological and vascular processes are at play:
Neurological basis
Nervous system imbalance: Migraines are seen as a disorder of brain excitability, involving a complex interplay of neurons, glia, and blood vessels.
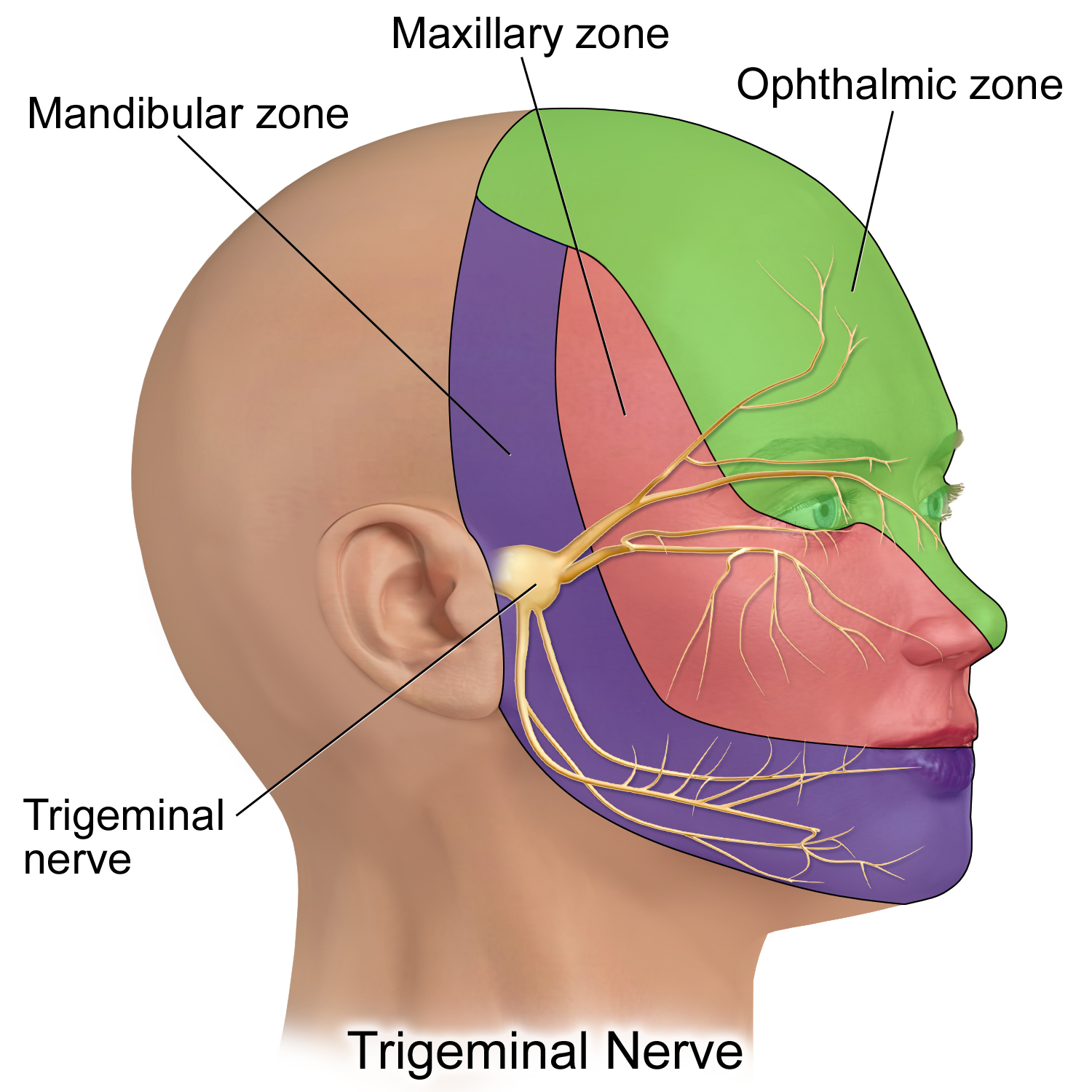
Trigeminovascular system: The trigeminovascular system, a network of nerves and blood vessels in the head, that innervates areas such as forehead, scalp, eyes, or neck, is activated during attacks and explains the throbbing, unilateral pain typical of migraines. (2,3). During a headache episode, the neck, the eyes and even the jaws can feel painful.
Neural pathways: Research shows specific brain regions are activated during headache attacks, pointing to a neurological cause.
Neurotransmitter imbalances: Serotonin, dopamine, and CGRP (calcitonin gene-related peptide) are key players (20) by influencing both pain perception and blood vessel function, thus highlighting the neurovascular connection (4,5). CGRP is released from sensory nerve endings in the trigeminovascular system and promotes neurogenic inflammation. It binds to CGRP receptors on blood vessels and immune cells, causing:
Vasodilation (widening of blood vessels in the meninges, contributing to the throbbing pain of migraines).
Increased permeability of blood vessels, allowing plasma proteins to leak into surrounding tissues, which triggers inflammation and pain
Sensitisation of pain receptors (nociceptors), lowering the threshold for pain signal transmission to the brain (4,5,7).
Genetic factors: Certain genetic conditions are known causes of migraine with aura and are rooted in neurological pathways.
Vascular involvement
Vasodilation and vasoconstriction: Historically, migraine was called a "vascular headache" due to the throbbing pain often caused by changes in blood vessel diameter, such as dilation and constriction (8).
Mediators: The vascular system plays a role by releasing and responding to various cytokines (inflammatory mediators) that can trigger nerve activation, further amplifying the pain symptoms.
Treatment targets: Some successful treatments act on the vasculature, highlighting the vascular component's importance in the disorder. That is why aspirin, a blood thinner, used to be prescribed and worked… but mostly went out of favour due to its gastrointestinal side effects and with the increasing popularity of paracetamol.
Understanding this neurovascular model helps shift the perspective from viewing migraines as "just a headache" to recognising them as a complex brain complaint with both neurological and vascular components. But is that the whole story and how these neurological processes get triggered in the first place?
2. Lifestyle Factors: How daily habits influence neurovascular health
Sleep and the Neurovascular System
Sleep disturbances—whether insomnia, poor quality, or irregular patterns—directly impact the neurovascular pathways involved in migraines. Sleep deprivation increases cortical excitability and disrupts the balance of neurotransmitters like serotonin and dopamine, which are critical for pain modulation and vascular regulation. Additionally, poor sleep elevates stress hormones (e.g., cortisol), which can sensitise the trigeminovascular system and lower the threshold for CGRP release, thereby increasing the chance for migraine attacks (9,10,12,15,19). For individuals prone to migraines, prioritising consistent, restorative sleep is not just about feeling rested, it’s about maintaining neurovascular stability.
Caffeine: A double-edged sword
Caffeine’s link with migraines is bidirectional. In moderate amounts, it may provide relief by constricting dilated blood vessels, thus reducing blood flow. However, it is not a long-term solution, nor is an effective one for everyone. Excessive intake or sudden withdrawal can trigger headaches by disrupting adenosine receptors and neurotransmitter balance, leading to rebound vasodilation and increased pain sensitivity (13). The key is consistency—abrupt changes in caffeine intake can destabilise the neurovascular system, making moderation and regularity important for those with migraine tendencies (13).
Stress and the HPA Axis: A central driver
Stress is perhaps the most significant lifestyle trigger for migraines, with up to 80% of sufferers reporting stress as a precipitating factor. Chronic stress activates the hypothalamic-pituitary-adrenal (HPA) axis, leading to prolonged cortisol release. Elevated cortisol sensitises the trigeminovascular system, promotes inflammation, and disrupts the balance of neurotransmitters like serotonin and CGRP—all of which lower the pain threshold. Stress also contributes to muscle tension (e.g., in the neck, scalp, jaws), which can further exacerbate headache intensity and duration. Importantly, migraines often occur not during peak stress but during the "letdown" period (e.g., weekends or holidays), when cortisol levels drop abruptly, triggering a neurovascular rebound effect (1, 12, 14, 15, 20).
Hydration and Blood Flow
Dehydration is a well-documented trigger for migraines and tension-type headaches. Even mild dehydration reduces blood volume and cerebral blood flow, increasing the risk of vasodilation and pain signal amplification in the trigeminovascular system. Adequate hydration helps maintain vascular stability and supports the brain’s ability to regulate pain pathways (15).
Diet, Blood Sugar, and Neurovascular Stability
Blood Sugar Fluctuations:
Hypoglycaemia or rapid changes in glucose levels (e.g., skipping meals) can activate the trigeminovascular system and prompt CGRP secretion, linking dietary habits to migraine attacks. Fluctuations in blood sugar—whether from skipping meals or consuming high-glycemic foods—can trigger migraines by disrupting neurotransmitter function and promoting vascular instability.(15, 21).
Alcohol and Vasodilators:
Alcohol (especially red wine) and vasodilatory substances (e.g., nitroglycerin, certain foods like aged cheese) can directly stimulate CGRP release from perivascular trigeminal nerves, leading to vasodilation and pain (21).
3. Physiological Factors: Connecting the dots
The HPA Axis and Neurovascular Sensitivity
The HPA axis doesn’t just respond to stress—it also influences the neurovascular pathways involved in migraines. Chronic stress and elevated cortisol (via the hypothalamic-pituitary-adrenal (HPA) axis) sensitise the trigeminovascular system, lowering the threshold for CGRP release. Stress-induced neurotransmitter imbalances (e.g., serotonin depletion) further amplify this response (20). Chronic HPA axis activation leads to central sensitisation, a state where the brain becomes hyper-responsive to pain signals. This sensitisation affects both the trigeminovascular system and the brain’s pain-processing centres, making individuals more susceptible to migraine attacks. Over time, this can create a cycle where stress, poor sleep, and dietary triggers more easily tip the balance toward pain. (20).
Liver Health and Toxin Clearance
The liver plays a crucial role in metabolising hormones, toxins, and medications that could otherwise contribute to neurovascular dysfunction. When the liver is overburdened—by poor diet, alcohol, environmental toxins, or medications—it struggles to clear these substances efficiently. This can lead to systemic inflammation and oxidative stress, both of which sensitise the trigeminovascular system and increase migraine susceptibility.
The Gut-Brain Axis
Emerging research highlights the gut’s role in migraine pathophysiology. The gut microbiome influences inflammation, neurotransmitter production, and even vascular function. Dysbiosis (microbial imbalance) and increased intestinal permeability ("leaky gut") can trigger systemic inflammation, which in turn sensitises the trigeminovascular system. Addressing gut health may therefore help modulate neurovascular responses and reduce migraine frequency. (21).
Hormonal Fluctuations
Oestrogen fluctuations (e.g., during menstruation, perimenopause) modulate CGRP secretion, explaining why migraines are often linked to hormonal cycles in women. Oestrogen withdrawal, after ovulation for instance, is associated with increased CGRP release (22).
Mitochondrial Dysfunction: A Hidden Driver of Migraines
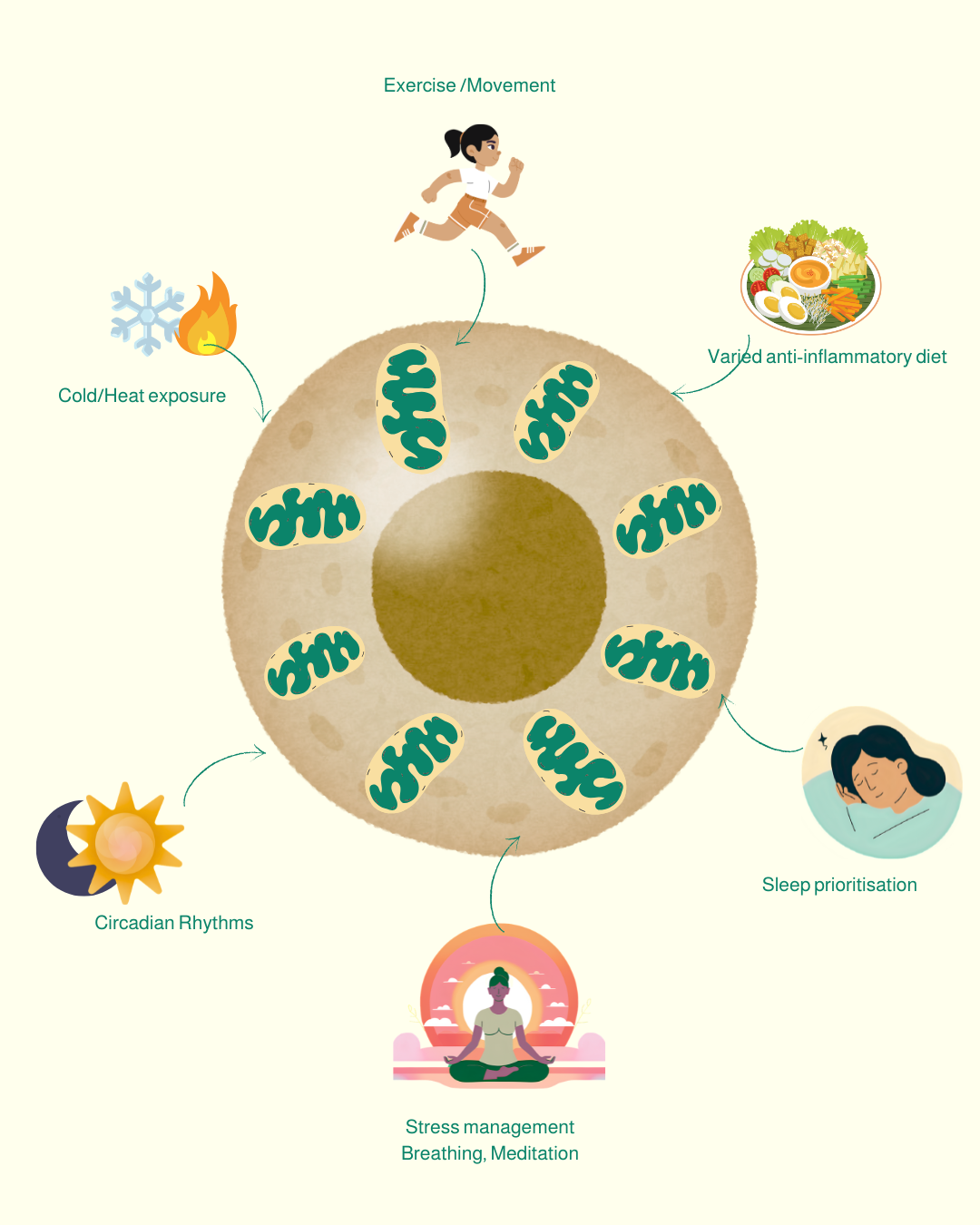
Emerging research confirms that brain mitochondrial dysfunction is a significant, yet often overlooked, mechanism underlying migraines. Mitochondria are special organelles of cells, responsible for producing energy required for neuronal and vascular function. In migraines, if mitochondria are dysfunctional, it means they cannot produce enough energy efficiently and they accumulate harmful free radicals, in other words "waste" that increases inflammation. These disturbances increase the brain's susceptibility to triggers like stress, sleep deprivation, or dietary factors.
There are many contributing factors to the “common“ headaches, which makes a whole-body approach the only approach to a long-term resolution.
4. Nutritional and Herbal Support for Neurovascular Health
Certain nutrients and herbs have been shown to support the neurovascular pathways involved in migraines.
These include, but are not limited to:
Magnesium helps regulate neurotransmitter release and vascular tone, supports mitochondrial function,
Antioxidants like quercetin or anthocyanidins (dietary and/or as supplements) reduce oxidative stress in both neurons and blood vessels.
Stress management and adaptogenic herbs like Withania, aka Ashwagandha, help the body to modulate the stress response and may help stabilise the neurovascular system by lowering cortisol and reducing inflammation (28, 31).
Dietary strategies and hepato-supportive supplements, including milk thistle, support liver detoxification, indirectly reducing the burden of toxins that could sensitise neurovascular pathways (26, 32). While these supplements are not cures, they can be valuable tools in a broader, holistic approach to managing migraines and headaches.
5. Integrating Lifestyle and Physiology: A personalised approach
The neurovascular nature of migraines means that effective management requires attention to both neurological and vascular health. Lifestyle factors like prioritising sleep, managing stress, identifying dietary triggers, and ensuring good hydration are not just peripheral concerns—they directly influence the physiological pathways that drive migraine attacks. Similarly, managing stress is about emotional well-being and is also about protecting the HPA axis and trigeminovascular system from chronic overactivation.
Movement and Exercise
If supplements can support mitochondrial function, only exercise and lifestyle factors can make new mitochondria. Regular, moderate activity (especially interval training) signals mitochondria to grow and adapt, while a sedentary lifestyle accelerates their decline.
Sleep Optimisation
Quality sleep is non-negotiable for mitochondrial repair, brain detoxification, stress management. Poor sleep disrupts mitochondria's detoxification and energy-replenishment cycles, worsening fatigue and oxidative stress.
For individuals prone to migraines, the most impactful changes often come from identifying and addressing their unique triggers. Some may find that stress management and sleep hygiene are most critical, while others may benefit more from dietary adjustments or liver support. The key is recognising that migraines are a whole-body issue, not just a neurovascular issue —and that small, consistent changes in daily habits can have profound effects on neurovascular health. You know yourself best, so if you have tried all the "right things" but headaches are still a chronic issue for you, you can work with me to guide you and help you navigate behaviours and obstacles.
References
Migraine Pathophysiology
1. Borsook, D., & Burstein, R. (2012). Migraine: Maladaptive brain responses to stress. Neuroscientist, 18(2), 166–181. https://doi.org/10.1177/1073858411409164 pmc.ncbi.nlm.nih.gov
2.Charles, A. (2018). Migraine: A brain disorder involving altered sensory, limbic, and homeostatic processing. Continuum (Minneapolis, Minn.), 24(4), 947–962. https://doi.org/10.1212/CON.0000000000000628 continuum.aan.com
3.Diener, H. C., Kurth, T., & Dodick, D. (2007). Patent foramen ovale and migraine. Current Pain and Headache Reports, 11(4), 236–240. https://doi.org/10.1007/s11916-007-0196-2 pmc.ncbi.nlm.nih.gov
4.Goadsby, P. J., Holland, P. R., Martins-Oliveira, M., Hoffmann, J., Schankin, C., & Akerman, S. (2017). Pathophysiology of migraine: A disorder of sensory processing. Physiological Reviews, 97(2), 553–622. https://doi.org/10.1152/physrev.00034.2015 journals.physiology.org
5.Noseda, R., & Burstein, R. (2013). Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, and neurogenic inflammation. Pain, 154(Suppl 1), S44–S53. https://doi.org/10.1016/j.pain.2013.07.021 jneurosci.org
6.Steiner, T. J., Stovner, L. J., Birbeck, G. L., Martelletti, P., & Jensen, R. (2019). The global burden of headache: Updates from the Global Burden of Disease Study 2016. Journal of Headache and Pain, 20(1), 1–12. https://doi.org/10.1186/s10194-019-0960-9 ncbi.nlm.nih.gov
7.Dodick, D. W. (2018). A phase-by-phase review of migraine pathophysiology. Headache: The Journal of Head and Face Pain, 58(4), 426–434. https://doi.org/10.1111/head.13300 headachejournal.onlinelibrary.wiley.com
8.Goadsby, P. J., Edvinsson, L., & Ekman, R. (1990). Release of vasoactive peptides in the extracerebral circulation of humans during migraine headache. Annals of Neurology, 28(2), 183–187. https://doi.org/10.1002/ana.410280210 frontiersin.org
Lifestyle and Physiological Factors
9. Bertisch, S. M., Li, W., Buettner, C., Raines, J., & Buxton, O. M. (2020). Nightly sleep duration, fragmentation, and quality and daily risk of migraine. Neurology, 94(12), e489–e496. https://doi.org/10.1212/WNL.0000000000009170 thelancet.com
10. Boardman, H. F., Thomas, E., Millson, D. S., & Croft, P. R. (2005). Psychological, sleep, lifestyle, and comorbid associations with headache. Headache, 45(7), 657–669. https://doi.org/10.1111/j.1526-4610.2005.05159.x nature.com
11. Gourley, L. M. (1997). A double-blind provocative study of chocolate as a trigger of headache. Cephalalgia, 17(8), 855–862. https://doi.org/10.1046/j.1468-2982.1997.1708855.x ccjm.org
12. Houle, T. T., Butschek, R. A., Turner, D. P., Smits, S. E., & Davenport, C. L. (2012). Stress and sleep duration predict headache severity in chronic headache sufferers. Pain, 153(12), 2432–2444. https://doi.org/10.1016/j.pain.2012.08.004 nature.com
13. Mostofsky, E., Mittleman, M. A., Buettner, C., May, A., & Schürks, M. (2020). Prospective cohort study of caffeinated beverage intake as a potential trigger of headaches among migraineurs. Headache, 60(3), 512–524. https://doi.org/10.1111/head.13734 pmc.ncbi.nlm.nih.gov
14. Pascoe, M. C., Thompson, D. R., Jenkins, Z. M., & Ski, C. F. (2017). Mindfulness mediates the physiological markers of stress: Systematic review and meta-analysis. Psychiatry Research, 259, 219–226. https://doi.org/10.1016/j.psychres.2017.10.013 thelancet.com
15. Robblee J. & Starling A. J. (2019). SEEDS for success: Lifestyle management in migraine. Cleveland Clinic Journal of Medicine, 86 (11) 741-749. https://doi.org/10.3949/ccjm.86a.19009
16. Roehrs, T., & Roth, T. (2015). Sleep and pain: Interaction of two vital functions. Sleep Medicine Reviews, 24, 61–72. https://doi.org/10.1016/j.smrv.2014.11.007 nature.com
17. Schürks, M., Rist, P. M., Bigal, M. E., Buring, J. E., Lipton, R. B., & Kurth, T. (2009). Migraine and cardiovascular disease: Systematic review and meta-analysis. BMJ, 339, b3914. https://doi.org/10.1136/bmj.b3914 sciencedirect.com
18. Stovner, L. J., Nichols, E., Steiner, T. J., Abd-Allah, F., Abdelalim, A., Al-Raddadi, R. M., ... & Katsarava, Z. (2018). Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet Neurology, 17(11), 954–976. https://doi.org/10.1016/S1474-4422(18)30322-3
19. Vgontzas, A. N., & Kales, A. (1999). Sleep and its disorders. Annual Review of Medicine, 50, 387–400. https://doi.org/10.1146/annurev.med.50.1.387 pmc.ncbi.nlm.nih.gov
20. McEwen, B. S. (2004). Protective and damaging effects of stress mediators. New England Journal of Medicine, 351(1), 33–41. https://doi.org/10.1056/NEJMra022116 thejournalofheadacheandpain.biomedcentral.com
21. Arzani, M., Jahromi, S. R., Ghorbani, Z., Vacante, M., Vacante, M., & Vacante, M. (2020). Gut-brain axis and migraine headache: A comprehensive review. The Journal of Headache and Pain, 21(1), 15. https://doi.org/10.1186/s10194-020-1078-9
22. Ruschel, M. A. P., & De Jesus, O. (2024). Migraine headache. StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560787/
23. Gross, E. C., et al. (2019). Metabolic changes and mitochondrial dysfunction in migraine patients. Journal of Headache and Pain, 20(1), 65. https://doi.org/10.1186/s10194-019-1015-2
Nutritional and Herbal Support
24. Amiri, P., Kazeminasab, S., Nejadghaderi, S. A., Mohammadinasab, R., Pourfathi, H., Araj-Khodaei, M., ... & Safiri, S. (2022). Migraine: a review on its history, global epidemiology, risk factors, and comorbidities. Frontiers in neurology, 12, 800605.
25. Ariyanfar, S., Razeghi Jahromi, S., Togha, M., & Ghorbani, Z. (2022). The efficacy of herbal supplements and nutraceuticals for prevention of migraine: Can they help? Nutritional Neuroscience, 25(9), 1801–1812. https://doi.org/10.1080/1028415X.2021.1904542 pubmed.ncbi.nlm.nih.gov
26. Bethesda (2020). LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases. https://www.ncbi.nlm.nih.gov/books/NBK548817/ ncbi.nlm.nih.gov
27. Chen, Y. S., Lee, H. F., Tsai, C. H., Hsu, Y. Y., Fang, C. J., Chen, C. J., & Hung, Y. H. (2022). Effect of vitamin B2 supplementation on migraine prophylaxis: A systematic review and meta-analysis. Nutritional Neuroscience, 25(9), 1801–1812. https://doi.org/10.1080/1028415X.2021.1904542
28. Lopresti, A. L., Smith, S. J., Malvi, H., & Kodgule, R. (2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract: A randomized, double-blind, placebo-controlled study. Medicine, 98(37), e17186. https://doi.org/10.1097/MD.0000000000017186 pubmed.ncbi.nlm.nih.gov
29. Parohan, M., Sarraf, P., Javanbakht, M. H., Ranji-Burachaloo, S., & Djalali, M. (2020). Effect of coenzyme Q10 supplementation on clinical features of migraine: A systematic review and dose-response meta-analysis of randomized controlled trials. Nutritional Neuroscience, 23(11), 868–875. https://doi.org/10.1080/1028415X.2019.1572940 pubmed.ncbi.nlm.nih.gov
30. Thompson, D. F., & Saluja, H. S. (2017). Prophylaxis of migraine headaches with riboflavin: A systematic review. Journal of Clinical Pharmacy and Therapeutics, 42(3), 394–398. https://doi.org/10.1111/jcpt.12548 americanmigrainefoundation.org
31. Sarris, J., Byrne, G. J., Stough, C., Bousman, C., Mischer, S., & Scholey, A. (2013). Clinical efficacy of Withania somnifera (ashwagandha) in stress and anxiety: A systematic review and meta-analysis. Complementary Therapies in Medicine, 21(4), 337–348. https://doi.org/10.1016/j.ctim.2013.05.003 sciencedirect.com
32. Rambaldi, A., Jacobs, B. P., & Gluud, C. (2007). Milk thistle for alcoholic and/or hepatitis B or C virus liver diseases. Cochrane Database of Systematic Reviews, 4, CD003620. https://doi.org/10.1002/14651858.CD003620.pub3 ncbi.nlm.nih.gov